Main Model
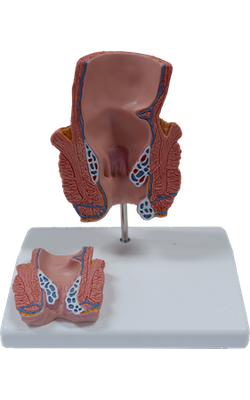
Relief : Haemorrhoids stage IV

Internal hemorrhoids (piles) are prolapses of rectal mucosa (more specifically, of the “anal cushions”) containing the normally dilated veins of the internal rectal venous plexus. Internal hemorrhoids result from a breakdown of the muscularis mucosae, a smooth muscle layer deep to the mucosa. Internal hemorrhoids that prolapse into or through the anal canal are often compressed by the contracted sphincters, impeding blood flow. As a result, they tend to strangulate and ulcerate. Because of the presence of abundant arteriovenous anastomoses, bleeding from internal hemorrhoids is characteristically bright red. The current practice is to treat only prolapsed, ulcerated internal hemorrhoids.
External hemorrhoids are thromboses (blood clots) in the veins of the external rectal venous plexus and are covered by skin. Predisposing factors for hemorrhoids include pregnancy, chronic constipation and prolonged toilet sitting and straining, and any disorder that impedes venous return, including increased intra-abdominal pressure.
The anastomoses between the superior, middle, and inferior rectal veins form clinically important communications between the portal and systemic venous systems. The superior rectal vein drains into the inferior mesenteric vein, whereas the middle and inferior rectal veins drain through the systemic system into the inferior vena cava. Any abnormal increase in pressure in the valveless portal system or veins of the trunk may cause enlargement of the superior rectal veins, resulting in an increase in blood flow or stasis in the internal rectal venous plexus. In the portal hypertension that occurs in relation to hepatic cirrhosis, the portocaval anastomosis between the superior and the middle and inferior rectal veins, along with portocaval anastomoses elsewhere, may become varicose. It is important to note that the veins of the rectal plexuses normally appear varicose (dilated and tortuous), even in newborns, and that internal hemorrhoids occur most commonly in the absence of portal hypertension.
Regarding pain from and the treatment of hemorrhoids, it is important to note that the anal canal superior to the pectinate line is visceral; thus it is innervated by visceral afferent pain fibers, so that an incision or needle insertion in this region is painless. Internal hemorrhoids are not painful and can be treated without anesthesia. Inferior to the pectinate line, the anal canal is somatic, supplied by the inferior anal (rectal) nerves containing somatic sensory fibers. Therefore, it is sensitive to painful stimuli (e.g., to the prick of a hypodermic needle). External hemorrhoids can be painful but often resolve in a few days.