Main Model

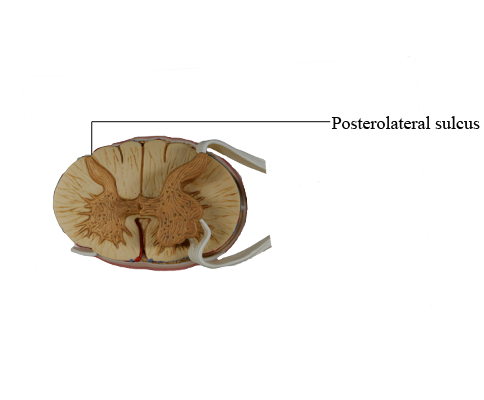
Top : Posterolateral sulcus
Although small in diameter, the spinal cord is the most important conduit between the body and the brain. It conveys sensory input from the arms, trunk, legs, and most of the viscera and contains fibers and cells that control the motor elements found in these structures. Consequently, injury to the spinal cord, especially at cervical levels, may cause permanent and catastrophic deficits or death.
Overview
The spinal cord participates in four essential functions. First, it receives primary sensory input from receptors in skin, skeletal muscles, and tendons (somatosensory fibers) and from receptors in thoracic, abdominal, and pelvic viscera (viscerosensory fibers). This sensory input may participate in spinal reflexes, be conveyed to higher levels of the neuraxis, or both.
Second, the spinal cord contains somatic motor neurons that innervate skeletal muscles and visceral motor neurons that, after synapsing in peripheral ganglia, influence smooth and cardiac muscle and glandular epithelium. Any disease process that damages the somatic motor neuron (as in poliomyelitis), compromises its ability to elicit a response in the skeletal muscle (as in myasthenia gravis), or affects both descending fibers and lower motor neurons (as in amyotrophic lateral sclerosis, also called Lou Gehrig disease) will result in weakness or paralysis.
Third, somatosensory fibers enter the spinal cord and influence anterior horn motor neurons either directly or indirectly through interneurons. These activated motor neurons, in turn, produce rapid involuntary contractions of skeletal muscles. The sensory fiber, the associated motor neuron, and the resultant involuntary muscle contraction constitute the circuit of the spinal reflex. Reflexes are essential to normal function and can be used as diagnostic tools to assess the functional integrity of the spinal cord.
Fourth, the spinal cord contains descending fibers that influence the activity of spinal neurons. These fibers originate in the cerebral cortex and brainstem, and damage to them adversely influences the activity of spinal motor and sensory neurons. In many cases the position of a lesion in the brainstem or spinal cord may give rise to a predictable or characteristic series of deficits, such as in decorticate rigidity or an alternating hemianesthesia.
In addition, injury to peripheral nerves will result in motor or sensory deficits distal to the lesion. These are most noticeable in the extremities and may be manifested as motor deficits (flaccid paralysis), a significant decrease or loss of essential spinal reflexes (hyperreflexia, hyporeflexia, areflexia), a loss of sensation (anesthesia), or abnormal sensations (paresthesia).
Spinal Cord Structure
The adult spinal cord is composed of a butterfly-shaped central area of neuron cell bodies, the gray matter, and a surround of myelinated and unmyelinated fibers, the white matter. Although the cavity of the neural tube was prominent during development, this space is a small ependyma-lined central canal in the adult spinal cord.
Surface Features
The human spinal cord extends from the foramen magnum to the level of the first or second lumbar vertebra. It consists of 8 cervical, 12 thoracic, 5 lumbar, and 5 sacral levels plus 1 coccygeal level. Although it is generally cylindric, the cord has cervical (C4 to T1) and lumbosacral (L1 to S2) enlargements, which serve, respectively, the upper and lower extremities.
There are eight cervical roots (and spinal cord levels) but only seven cervical vertebrae. So how do the roots relate to their corresponding vertebrae? The C1 root is located between the base of the skull and the C1 vertebra. Therefore roots C1 through C7 are located above (rostral to) their respectively numbered vertebrae, and the C8 root is located between the C7 and T1 vertebrae. Beginning with the T1 vertebra and extending caudally, all roots are located caudal to their respectively numbered vertebrae. It is also important to remember that each level or segment of the spinal cord is specified by the intervertebral foramen through which the posterior and anterior roots originating from that cord level exit.
There are few superficial markings on the spinal cord. The posterior median sulcus separates the posterior portion of the cord into halves and contains a delicate layer of pia, the posterior median septum. The posterolateral sulcus, which runs the full length of the cord, represents the entry point of posterior root (sensory) fibers. This area is frequently called the posterior (dorsal) root entry zone. In cervical and upper thoracic regions, a posterior intermediate sulcus and septum are found between the posterolateral and posterior median sulci. This sulcus and septum are insinuated between the medially located gracile fasciculus and the laterally located cuneate fasciculus. Because of the organization of the gracile and cuneate fasciculi, the posterior intermediate septum is present only in upper thoracic and cervical cord levels.
On the anterolateral surface of the spinal cord, the anterolateral sulcus is the exit point for anterior root (motor) fibers. Because the anterior roots exit in a somewhat irregular pattern, this sulcus is not as distinct as the posterolateral sulcus.
The anterior median fissure is a prominent space dividing the anterior part of the cord into halves. This fissure contains delicate strands of pia and, more important, the sulcal branches of the anterior spinal artery.
Spinal Meninges
The tubular dural sac that encloses the spinal cord is attached cranially to the rim of the foramen magnum, and its closed caudal end is anchored to the coccyx by the filum terminale externum. This dural sac is separated from the vertebrae by the epidural space. The spinal cord, in turn, is attached to the dural sac by the laterally placed denticulate ligaments and b the filum terminale internum. This latter structure extends caudally from the end of the spinal cord, the conus medullaris, and terminates in the attenuated (closed) portion of the dural sac, which is located adjacent to the S2 vertebra. The filum terminale externum extends caudally from the closed dural sac to its attachment on the inner aspect of the coccyx.
The arachnoid mater adheres to the inner surface of the dura mater, and the pia mater is intimately attached to the surface of the cord. The subarachnoid space between these layers is continuous with the subarachnoid space around the brain and is likewise filled with cerebrospinal fluid. In adults the conus medullaris is located at the level of the L1 or L2 vertebral body. Extending caudally from this point to the end of the dural sac is an enlarged part of the spinal subarachnoid space, the lumbar cistern. This cistern contains the posterior and anterior roots from spinal segments L2 to Coc1 as they sweep caudally. Collectively, these roots form the cauda equina. The method of choice to obtain a sample of cerebrospinal fluid for diagnostic purposes is the lumbar puncture (spinal tap), in which a largebore needle is introduced between the L3 and L4 or L4 and L5 vertebral arches into the lumbar cistern.
White Matter
The white matter of the spinal cord is divided into three large regions, each of which is composed of individual tracts or fasciculi. The posterior funiculus is located between the posterior median septum and the medial edge of the horn. At cervical levels, this area consists of the gracile and cuneate fasciculi; collectively, these are commonly referred to as the posterior columns.
The lateral funiculus is the area of white matter located between the posterolateral and anterolateral sulci. This region of the cord contains clinically important ascending and descending tracts. Those most important in diagnosis of the neurologically impaired patient are the lateral corticospinal tract and the anterolateral system (ALS).
Located between the anterolateral sulcus and the ventral median fissure is a comparatively small region, the anterior funiculus. This area contains reticulospinal and vestibulospinal fibers, portions of the ALS, the anterior corticospinal tract, and a composite bundle called the medial longitudinal fasciculus (MLF).
Two small but important components of the white matter are the anterior white commissure and the posterolateral (dorsolateral) tract. The anterior white commissure is located on the anterior midline and is separated from the central canal by a narrow band of small cells. The posterolateral tract, the tract of Lissauer, is a small bundle of lightly myelinated and unmyelinated fibers capping the posterior horn.
Gray Matter
The gray matter of the spinal cord is composed of neuron cell bodies, their dendrites and the initial part of the axon, the axon terminals of fibers synapsing in this area, and glial cells. Because this area has few myelinated fibers, it appears distinctly light and has a characteristic shape in myelin-stained sections.
The spinal gray matter is divided into a posterior (dorsal) horn, an anterior (ventral) horn, and the region where these meet, commonly called the intermediate zone (or intermediate gray). On the basis of the shape, size, and distribution of neurons located in these areas, the gray matter is divided into laminae (Rexed laminae) I to IX and an area X around the central canal. These laminae are also characterized by the input they receive and the trajectory of axons originating from each lamina.
The posterior horn is composed of laminae I to VI. The most distinct structure in the posterior horn, the substantia gelatinosa (lamina II), is capped by cells of the posteromarginal nucleus (lamina I). Laminae III to VI are located sequentially below the substantia gelatinosa. Laminae III and IV may also be called the nucleus proprius (posterior or dorsal proper sensory nucleus); their cells have elaborate dendrites that extend into lamina II. Laminae V and VI, which form the base of the posterior horn, are usually divided into medial and lateral portions.
The intermediate zone, lamina VII, extends from the area of the central canal to the lateral edge of the spinal gray and varies in shape at different levels of the cord. Particularly characteristic of lamina VII at thoracic levels are the posterior thoracic nucleus (dorsal nucleus of Clarke) and the lateral horn, which contains the intermediolateral nucleus, frequently called the intermediolateral cell column.
The anterior horn is made up of laminae VIII and IX. Lamina VIII contains a population of smaller cells that are interneurons and tract cells. Lamina IX consists of several distinct clusters of large motor neurons whose axons directly innervate skeletal muscle.
Blood Supply
The blood supply to the spinal cord is derived from the anterior and posterior spinal arteries and from branches of segmental arteries. The segmental branches that serve the posterior and anterior roots and the posterior root ganglia are the radicular arteries, and branches that largely bypass the roots to supplement the blood supply to the cord are the spinal medullary arteries. One especially large spinal medullary artery, the artery of Adamkiewicz, is most often seen at L2 on the left. This vessel is an important source of blood supply to the cord and must be preserved during surgery in this area. At each level, terminal branches of the spinal medullary arteries join to form an arterial network, the arterial vasocorona, on the surface of the spinal cord.
The posterior columns and peripheral parts of the lateral and anterior funiculi are served by the posterior spinal arteries and arterial vasocorona. Most of the gray matter and the adjacent parts of the white matter are served by the central branches of the anterior spinal artery. These central branches tend to alternate: one serves the left side of the cord, the next serves the right side.
Trauma, as in hyperextension of the cervical spine or mechanical injury to the cord, may cause occlusion or spasm of the anterior spinal artery. The result is bilateral damage to the cervical cord (central cervical cord syndrome). The characteristic features of this syndrome are bilateral weakness of the extremities, primarily evident in the arms, forearms, and hands; a patchy loss of sensation below the lesion; and urinary retention.