Main Model

Fistula
Anal Fissures; Ischio-anal and
Peri-anal Abscesses
The ischio-anal fossae are occasionally the sites of
infection, which may result in the formation of
ischio-anal abscesses. These collections of pus are painful. Infections may reach the ischio-anal
fossae in several ways:
• After cryptitis (inflammation of anal sinuses).
• Extension from a pelvirectal abscess.
• After a tear in the anal mucous membrane.
• From a penetrating wound in the anal region.
Diagnostic signs of an ischio-anal abscess are fullness and
tenderness between the anus and the ischial tuberosity. A
peri-anal abscess may rupture spontaneously, opening into
the anal canal, rectum, or peri-anal skin. Because the ischio-anal fossae communicate posteriorly through the deep post-anal space, an abscess in one fossa may spread to the other
one, and form a semicircular "horseshoe-shaped" abscess
around the posterior aspect of the anal canal.
In chronically constipated persons, the anal valves and
mucosa may be torn by hard feces. An anal fissure (slit-like
lesion) is usually located in the posterior midline, inferior to the anal valves. It is painful because this region is supplied by
sensory fibers of the inferior rectal nerves. A peri-anal abscess
may follow infection of an anal fissure, and the infection may spread to the ischio-anal fossae and form ischio-anal abscesses
or spread into the pelvis and form a pelvirectal abscess.
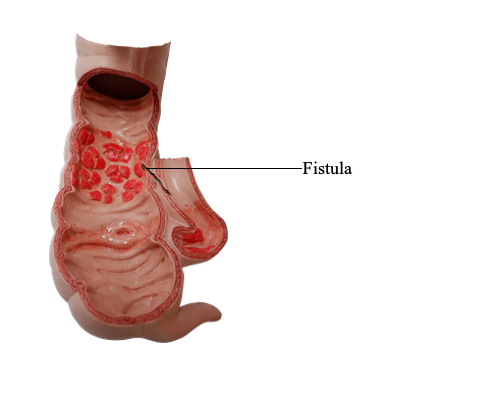
An anal fistula may result from the spread of an anal infection and cryptitis (inflammation of an anal sinus). One end of
this abnormal canal (fistula) opens into the anal canal, and
the other end opens into an abscess in the ischio-anal fossa
or into the peri-anal skin.