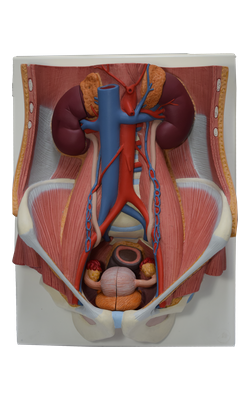
Main Model
9 Prostate
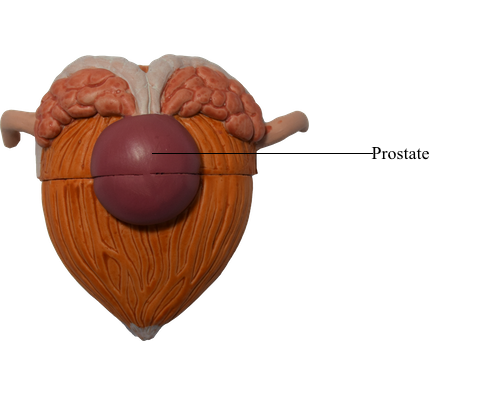
The prostate (approximately 3 cm long, 4 cm wide, and 2 cm in antero-posterior [AP] depth) is the largest accessory gland of the male reproductive system. The firm, walnut-size prostate surrounds the prostatic urethra. The glandular part makes up approximately two thirds of the prostate; the other third is fibromuscular.
The fibrous capsule of the prostate is dense and neurovascular, incorporating the prostatic plexuses of veins and nerves. All this is surrounded by the visceral layer of the pelvic fascia, forming a fibrous prostatic sheath that is thin anteriorly, continuous anterolaterally with the puboprostatic ligaments, and dense posteriorly where it blends with the rectovesical septum.
The prostate has:
• A base closely related to the neck of the bladder.
• An apex that is in contact with fascia on the superior aspect of the urethral sphincter and deep perineal muscles.
• A muscular anterior surface, featuring mostly transversely oriented muscle fibers forming a vertical, trough-like hemisphincter (rhabdosphincter), which is part of the urethral sphincter. The anterior surface is separated from the pubic symphysis by retroperitoneal fat in the retropubic space.
• A posterior surface that is related to the ampulla of the rectum.
• Inferolateral surfaces that are related to the levator ani.
Although not clearly distinct anatomically, the following lobes of the prostate are traditionally described:
• The isthmus of the prostate (commissure of prostate; historically, the anterior “lobe”) lies anterior to the urethra. It is fibromuscular, the muscle fibers representing a superior continuation of the external urethral sphincter muscle to the neck of the bladder, and contains little, if any, glandular tissue.
• Right and left lobes of the prostate, separated anteriorly by the isthmus and posteriorly by a central, shallow longitudinal furrow, may each be subdivided for descriptive purposes into four indistinct lobules defined by their relationship to the urethra and ejaculatory ducts, and - although less apparent - by the arrangement of the ducts and connective tissue:
(1) an inferoposterior (lower posterior) lobule that lies posterior to the urethra and inferior to the ejaculatory ducts. This lobule constitutes the aspect of the prostate palpable by digital rectal examination.
(2) an inferolateral (lower lateral) lobule directly lateral to the urethra, forming the major part of the right or left lobe.
(3) a superomedial lobule, deep to the inferoposterior lobule, surrounding the ipsilateral ejaculatory duct.
(4) an anteromedial lobule, deep to the inferolateral lobule, directly lateral to the proximal prostatic urethra.
An embryonic middle (median) lobe gives rise to (3) and (4) above. This region tends to undergo hormone-induced hypertrophy in advanced age, forming a middle lobule that lies between the urethra and the ejaculatory ducts and is closely related to the neck of the bladder. Enlargement of the middle lobule is believed to be at least partially responsible for the formation of the uvula that may project into the internal urethral orifice.
Some clinicians, especially urologists and sonographers, divide the prostate into peripheral and central (internal) zones. The central zone is comparable to the middle lobe.
The prostatic ducts (20-30) open chiefly into the prostatic sinuses that lie on either side of the seminal colliculus on the posterior wall of the prostatic urethra. Prostatic fluid, a thin, milky fluid, provides approximately 20% of the volume of semen (a mixture of secretions produced by the testes, seminal glands, prostate, and bulbo-urethral glands that provides the vehicle by which sperms are transported) and plays a role in activating the sperms.
The prostatic arteries are mainly branches of the internal iliac artery, especially the inferior vesical arteries, but also the internal pudendal and middle rectal arteries.
The veins join to form a plexus around the sides and base of the prostate. This prostatic venous plexus, between the fibrous capsule of the prostate and the prostatic sheath, drains into the internal iliac veins. The prostatic venous plexus is continuous superiorly with the vesical venous plexus and communicates posteriorly with the internal vertebral venous plexus.