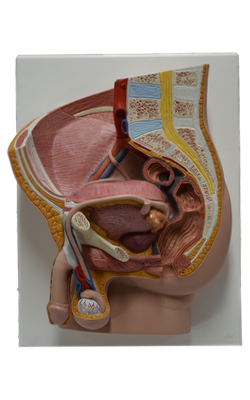
Main Model
Bulbospongiosus muscle
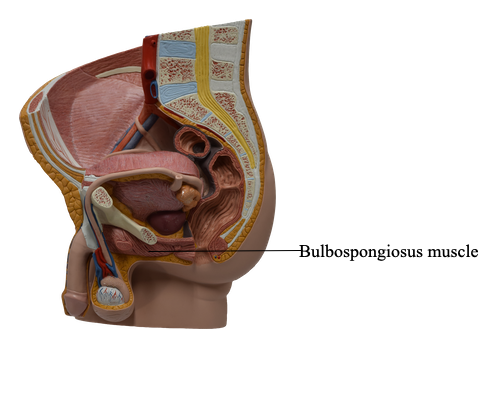
The root of the penis, the attached part, consists of the crura, bulb, and ischiocavernosus and bulbospongiosus muscles. The root is located in the superficial perineal pouch, between the perineal membrane superiorly and the deep perineal fascia inferiorly. The crura and bulb of the penis consist of erectile tissue. Each crus is attached to the inferior part of the internal surface of the corresponding ischial ramus, anterior to the ischial tuberosity. The enlarged posterior part of the bulb of the penis is penetrated superiorly by the urethra, continuing from its intermediate part.
The body of the penis is the free pendulous part that is suspended from the pubic symphysis. Except for a few fibers of the bulbospongiosus near the root of the penis and the ischiocavernosus that embrace the crura, the body of the penis has no muscles.
Perineal Muscles of Male
The superficial perineal muscles, located in the superficial perineal pouch, include the superficial transverse perineal, bulbospongiosus, and ischiocavernosus muscles.
The superficial transverse perineal muscles and the bulbospongiosus muscles join the external anal sphincter in attaching centrally to the perineal body. They cross the pelvic outlet like intersecting beams, supporting the perineal body to aid the pelvic diaphragm in supporting the pelvic viscera. Simultaneous contraction of the superficial perineal muscles (plus the deep transverse perineal muscle) during penile erection provides a firmer base for the penis.
The bulbospongiosus muscles form a constrictor that compresses the bulb of the penis and the corpus spongiosum, thereby aiding in emptying the spongy urethra of residual urine and/or semen. The anterior fibers of the bulbospongiosus, encircling the most proximal part of the body of the penis, also assist erection by increasing the pressure on the erectile tissue in the root of the penis. At the same time, they also compress the deep dorsal vein of the penis, impeding venous drainage of the cavernous spaces and helping promote enlargement and turgidity of the penis.
The ischiocavernosus muscles surround the crura in the root of the penis. They force blood from the cavernous spaces in the crura into the distal parts of the corpora cavernosa, which increases the turgidity (firm distension) of the penis during erection. Contraction of the ischiocavernosus muscles also compresses the tributaries of deep dorsal vein of the penis leaving the crus of the penis, thereby restricting venous outflow from the penis and helping maintain the erection.
Because of their function during erection and the activity of the bulbospongiosus subsequent to urination and ejaculation to expel the last drops of urine and semen, the perineal muscles are generally more developed in males than in females.
Erection, Emission, Ejaculation, and Remission
When a male is stimulated erotically, arteriovenous anastomoses by which blood is normally able to bypass the “empty” potential spaces or sinuses of the corpora cavernosa are closed. The smooth muscle in the fibrous trabeculae and coiled helicine arteries relaxes (is inhibited) as a result of parasympathetic stimulation (S2-S4 through the cavernous nerves from the prostatic nerve plexus). Consequently, the helicine arteries straighten, enlarging their lumina and allowing blood to flow into and dilate the cavernous spaces in the corpora of the penis.
The bulbospongiosus and ischiocavernosus muscles compress veins egressing from the corpora cavernosa, impeding the return of venous blood. As a result, the corpora cavernosa and corpus spongiosum become engorged with blood near arterial pressure, causing the erectile bodies to become turgid (enlarged and rigid), and an erection occurs.
During emission, semen (sperms and other glandular secretions) is delivered to the prostatic urethra through the ejaculatory ducts after peristalsis of the ductus deferentes and seminal glands. Prostatic fluid is added to the seminal fluid as the smooth muscle in the prostate contracts. Emission is a sympathetic response (L1-L2 nerves). During ejaculation, semen is expelled from the urethra through the external urethral orifice.
Ejaculation results from:
• Closure of the internal urethral sphincter at the neck of the urinary bladder, a sympathetic response (L1-L2 nerves).
• Contraction of the urethral muscle, a parasympathetic response (S2-S4 nerves).
• Contraction of the bulbospongiosus muscles, from the pudendal nerves (S2-S4).
After ejaculation, the penis gradually returns to a flaccid state (remission), resulting from sympathetic stimulation, which causes constriction of the smooth muscle in the coiled helicine arteries. The bulbospongiosus and ischiocavernosus muscles relax, allowing more blood to be drained from the cavernous spaces in the corpora cavernosa into the deep dorsal vein.
Bulbospongiosus
Origin:
Male: median raphe on ventral surface of bulb of penis; perineal body
Female: perineal body
Course and Distribution:
Male: surrounds lateral aspects of bulb of penis and most proximal part of body of penis, inserting into perineal membrane, dorsal aspect of corpus spongiosum and corpora cavernosa, and fascia of bulb of penis
Female: passes on each side of lower vagina, enclosing bulb and greater vestibular gland; inserts into pubic arch and fascia of corpora cavernosa of clitoris
Innervation: Muscular (deep) branch of perineal nerve, a branch of pudendal nerve (S2-S4)
Main Action(s):
Male: supports and fixes perineal body/pelvic floor; compresses bulb of penis to expel last drops of urine/semen; assists erection by compressing outflow via deep perineal vein and by pushing blood from bulb into body of penis
Female: supports and fixes perineal body/pelvic floor; “sphincter” of vagina; assists in erection of clitoris (and perhaps bulb of vestibule); compresses greater vestibular gland