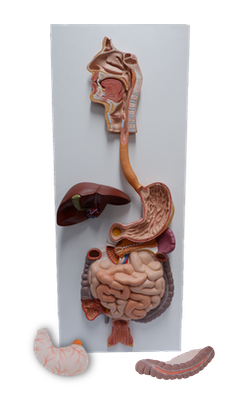
Main Model
Descending colon
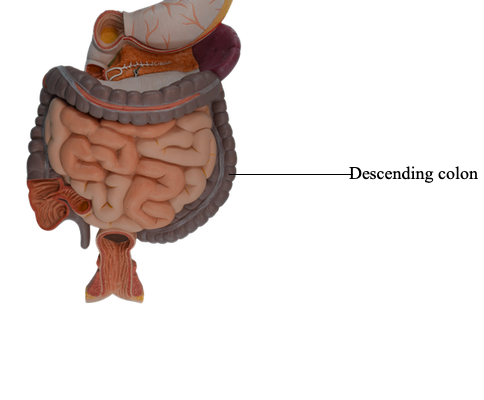
Colon
The colon has four parts - ascending, transverse, descending, and sigmoid - that succeed one another in an arch. The colon encircles the small intestine, the ascending colon lying to the right of the small intestine, the transverse colon superior and/or anterior to it, the descending colon to the left of it, and the sigmoid colon inferior to it.
The ascending colon is the second part of the large intestine. It passes superiorly on the right side of the abdominal cavity from the cecum to the right lobe of the liver, where it turns to the left at the right colic flexure (hepatic flexure). This flexure lies deep to the 9th and 10th ribs and is overlapped by the inferior part of the liver.
The ascending colon is narrower than the cecum and is secondarily retroperitoneal along the right side of the posterior abdominal wall. The ascending colon is usually covered by peritoneum anteriorly and on its sides; however, in approximately 25% of people, it has a short mesentery. The ascending colon is separated from the anterolateral abdominal wall by the greater omentum. A deep vertical groove lined with parietal peritoneum, the right paracolic gutter, lies between the lateral aspect of the ascending colon and the adjacent abdominal wall.
The arterial supply to the ascending colon and right colic flexure is from branches of the SMA, the ileocolic and right colic arteries. These arteries anastomose with each other and with the right branch of the middle colic artery, the first of a series of anastomotic arcades that is continued by the left colic and sigmoid arteries to form a continuous arterial channel, the marginal artery (juxtacolic artery). This artery parallels and extends the length of the colon close to its mesenteric border.
Venous drainage from the ascending colon flows through tributaries of the SMV, the ileocolic and right colic veins. The lymphatic drainage passes first to the epicolic and paracolic lymph nodes, next to the ileocolic and intermediate right colic lymph nodes, and from them to the superior mesenteric lymph nodes. The nerve supply to the ascending colon is derived from the superior mesenteric nerve plexus.
The transverse colon is the third, longest, and most mobile part of the large intestine. It crosses the abdomen from the right colic flexure to the left colic flexure, where it turns inferiorly to become the descending colon. The left colic flexure (splenic flexure) is usually more superior, more acute, and less mobile than the right colic flexure. It lies anterior to the inferior part of the left kidney and attaches to the diaphragm through the phrenicocolic ligament. The transverse colon and its mesentery, the transverse mesocolon, loops down, often inferior to the level of the iliac crests. The mesentery is adherent to or fused with the posterior wall of the omental bursa. The root of the transverse mesocolon lies along the inferior border of the pancreas and is continuous with the parietal peritoneum posteriorly. Being freely movable, the transverse colon is variable in position, usually hanging to the level of the umbilicus (L3 vertebral level). However, in tall thin people, the transverse colon may extend into the pelvis.
The arterial supply of the transverse colon is mainly from the middle colic artery, a branch of the SMA. However, the transverse colon may also receive arterial blood from the right and left colic arteries via anastomoses, part of the series of anastomotic arcades that collectively form the marginal artery (juxtacolic artery).
Venous drainage of the transverse colon is through the SMV. The lymphatic drainage of the transverse colon is to the middle colic lymph nodes, which in turn drain to the superior mesenteric lymph nodes.
The nerve supply of the transverse colon is from the superior mesenteric nerve plexus via the peri-arterial plexuses of the right and middle colic arteries. These nerves transmit sympathetic, parasympathetic (vagal), and visceral afferent nerve fibers.
The descending colon occupies a secondarily retroperitoneal position between the left colic flexure and the left iliac fossa, where it is continuous with the sigmoid colon. Thus, peritoneum covers the colon anteriorly and laterally and binds it to the posterior abdominal wall. Although retroperitoneal, the descending colon, especially in the iliac fossa, has a short mesentery in approximately 33% of people; however, it is usually not long enough to cause volvulus (twisting) of the colon. As it descends, the colon passes anterior to the lateral border of the left kidney. As with the ascending colon, the descending colon has a paracolic gutter (the left one) on its lateral aspect.
The sigmoid colon, characterized by its S-shaped loop of variable length, links the descending colon and the rectum. The sigmoid colon extends from the iliac fossa to the third sacral (S3) vertebra, where it joins the rectum. The termination of the teniae coli, approximately 15 cm from the anus, indicates the rectosigmoid junction.
The sigmoid colon usually has a long mesentery - the sigmoid mesocolon - and therefore has considerable freedom of movement, especially its middle part. The root of the sigmoid mesocolon has an inverted V-shaped attachment, extending first medially and superiorly along the external iliac vessels and then medially and inferiorly from the bifurcation of the common iliac vessels to the anterior aspect of the sacrum. The left ureter and the division of the left common iliac artery lie retroperitoneally, posterior to the apex of the root of the sigmoid mesocolon. The omental appendices of the sigmoid colon are long; they disappear when the sigmoid mesentery terminates. The teniae coli also disappear as the longitudinal muscle in the wall of the colon broadens to form a complete layer in the rectum.
The arterial supply of the descending and sigmoid colon is from the left colic and sigmoid arteries, branches of the inferior mesenteric artery. Thus, at approximately the left colic flexure, a second transition occurs in the blood supply of the abdominal part of the alimentary canal: the SMA supplying blood to that part orad (proximal) to the flexure (derived from the embryonic midgut), and the IMA supplying blood to the part aborad (distal) to the flexure (derived from the embryonic hindgut). The sigmoid arteries descend obliquely to the left, where they divide into ascending and descending branches. The superior branch of the most superior sigmoid artery anastomoses with the descending branch of the left colic artery, thereby forming a part of the marginal artery. Venous drainage from the descending colon and sigmoid colon is provided by the inferior mesenteric vein, flowing usually into the splenic vein and then the hepatic portal vein on its way to the liver.
Lymphatic drainage from the descending colon and sigmoid colon is conducted through vessels passing to the epicolic and paracolic nodes, and then through the intermediate colic lymph nodes along the left colic artery. Lymph from these nodes passes to the inferior mesenteric lymph nodes that lie around the IMA. However, lymph from the left colic flexure may also drain to the superior mesenteric lymph nodes.
Orad (toward the mouth, or proximal) to the left colic flexure, sympathetic and parasympathetic fibers travel together from the abdominal aortic plexus via peri-arterial plexuses to reach the abdominal part of the alimentary tract; however, aborad (away from the mouth, or distal) to the flexure, they follow separate routes.
The sympathetic nerve supply of the descending and sigmoid colon is from the lumbar part of the sympathetic trunk via lumbar (abdominopelvic) splanchnic nerves, the superior mesenteric plexus, and the peri-arterial plexuses following the inferior mesenteric artery and its branches.
The parasympathetic nerve supply is from the pelvic splanchnic nerves via the inferior hypogastric (pelvic) plexus and nerves, which ascend retroperitoneally from the plexus, independent of the arterial supply to this part of the gastrointestinal tract. Orad to the middle of the sigmoid colon, visceral afferents conveying pain sensation pass retrogradely with sympathetic fibers to thoracolumbar spinal sensory ganglia, whereas those carrying reflex information travel with the parasympathetic fibers to vagal sensory ganglia. Aborad to the middle of the sigmoid colon, all visceral afferents follow the parasympathetic fibers retrogradely to the sensory ganglia of spinal nerves S2-S4.