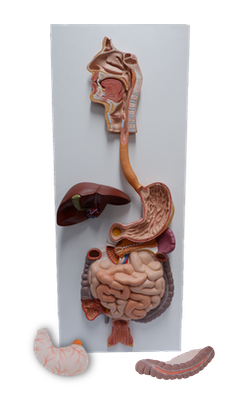
Main Model
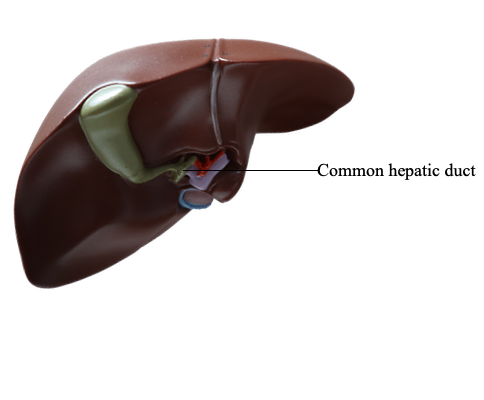
Common hepatic duct
Biliary Ducts
The biliary ducts convey bile from the liver to the duodenum. Bile is produced continuously by the liver and stored
and concentrated in the gallbladder, which releases it intermittently when fat enters the duodenum. Bile emulsifi es the
fat so that it can be absorbed in the distal intestine.
Normal hepatic tissue, when sectioned, is traditionally
described as demonstrating a pattern of hexagonal-shaped
liver lobules (Fig. 2.69A) when viewed under low magnifi -
cation. Each lobule has a central vein running through its
center from which sinusoids (large capillaries) and plates
of hepatocytes (liver cells) radiate toward an imaginary
peri meter extrapolated from surrounding interlobular
portal triads (terminal branches of the hepatic portal vein
and hepatic artery and initial branches of the biliary ducts).
Although commonly said to be the anatomical units of the
liver, hepatic “lobules” are not structural entities; instead, the
lobular pattern is a physiological consequence of pressure
gradients and is altered by disease. Because the bile duct is
not central, the hepatic lobule does not represent a functional
unit like acini of other glands. However, the hepatic lobule
is a fi rmly established concept and is useful for descriptive
purposes.
The hepatocytes secrete bile into the bile canaliculi formed
between them. The canaliculi drain into the small interlobular
biliary ducts and then into large collecting bile ducts of the intrahepatic portal triad, which merges to form the hepatic ducts
(Fig. 2.69B). The right and left hepatic ducts drain the right
and left (parts of the) liver, respectively. Shortly after leaving the
porta hepatis, these hepatic ducts unite to form the common
hepatic duct, which is joined on the right side by the cystic
duct to form the bile duct (part of the extrahepatic portal triad of
the lesser omentum), which conveys the bile to the duodenum.
BILE DUCT
The bile duct (formerly called the common bile duct) forms
in the free edge of the lesser omentum by the union of the
cystic duct and common hepatic duct (Figs. 2.65 and 2.69B).
The length of the bile duct varies from 5 to 15 cm, depending on where the cystic duct joins the common hepatic duct.
The bile duct descends posterior to the superior part of
the duodenum and lies in a groove on the posterior surface
of the head of the pancreas. On the left side of the descending part of the duodenum, the bile duct comes into contact
with the main pancreatic duct. These ducts run obliquely
through the wall of this part of the duodenum, where they
unite, forming a dilation, the hepatopancreatic ampulla (Fig.
2.69C). The distal end of the ampulla opens into the duodenum through the major duodenal papilla (see Fig. 2.45C).
The circular muscle around the distal end of the bile duct is
thickened to form the sphincter of the bile duct (L. ductus choledochus) (Fig. 2.69C). When this sphincter contracts,
bile cannot enter the ampulla and the duodenum; hence, bile
backs up and passes along the cystic duct to the gallbladder
for concentration and storage.
The arterial supply of the bile duct is from the (Fig. 2.71):
• Cystic artery: supplying the proximal part of the duct.
• Right hepatic artery: supplying the middle part of the duct.
• Posterior superior pancreaticoduodenal artery and gastroduodenal artery: supplying the retroduodenal part of
the duct.
The venous drainage from the proximal part of the bile
duct and the hepatic ducts usually enter the liver directly
(Fig. 2.72). The posterior superior pancreaticoduodenal vein
drains the distal part of the bile duct and empties into the
hepatic portal vein or one of its tributaries.
The lymphatic vessels from the bile duct pass to the cystic
lymph nodes near the neck of the gallbladder, the lymph
node of the omental foramen, and the hepatic lymph
nodes (Figs. 2.70 and 2.71). Efferent lymphatic vessels from
the bile duct pass to the celiac lymph nodes.