Main Model
Hard palate
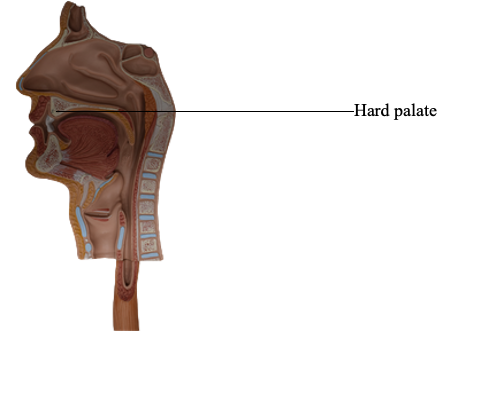
Palate
The palate forms the arched roof of the mouth and the floor
of the nasal cavities. It separates the oral cavity
from the nasal cavities and the nasopharynx, the part of the
pharynx superior to the soft palate. The superior (nasal) surface of the palate is covered with respiratory mucosa, and the
inferior (oral) surface is covered with oral mucosa, densely
packed with glands. The palate consists of two regions: the
hard palate anteriorly and the soft palate posteriorly.
Hard Palate
The hard palate is vaulted (concave); this space is mostly filled
by the tongue when it is at rest. The anterior two thirds of the
palate has a bony skeleton formed by the palatine processes
of the maxillae and the horizontal plates of the palatine bones. The incisive fossa is a depression in the midline
of the bony palate posterior to the central incisor teeth into
which the incisive canals open. The nasopalatine nerves pass
from the nose through a variable number of incisive canals and
foramina that open into the incisive fossa.
Medial to the 3rd molar tooth, the greater palatine foramen pierces the lateral border of the bony palate.
The greater palatine vessels and nerve emerge from this foramen and run anteriorly on the palate. The lesser palatine
foramina posterior to the greater palatine foramen pierce
the pyramidal process of the palatine bone. These foramina
transmit the lesser palatine nerves and vessels to the soft palate and adjacent structures.
Soft Palate
The soft palate is the movable posterior third of the palate
and is suspended from the posterior border of the hard palate. The soft palate has no bony skeleton;
however, its anterior aponeurotic part is strengthened by the
palatine aponeurosis, which attaches to the posterior edge
of the hard palate. The aponeurosis is thick anteriorly and
thin posteriorly, where it blends with a posterior muscular
part. Postero-inferiorly, the soft palate has a curved free margin from which hangs a conical process, the uvula.
When a person swallows, the soft palate initially is tensed
to allow the tongue to press against it, squeezing the bolus
of food to the back of the mouth. The soft palate is then elevated posteriorly and superiorly against the wall of the pharynx, thereby preventing passage of food into the nasal cavity.
Laterally, the soft palate is continuous with the wall of
the pharynx and is joined to the tongue and pharynx by the
palatoglossal and palatopharyngeal arches, respectively. A few taste buds are located in the epithelium
covering the oral surface of the soft palate, the posterior wall
of the oropharynx, and the epiglottis.
The fauces (Latin throat) is the space between the oral cavity
and the pharynx. The fauces is bounded superiorly by the soft
palate, inferiorly by the root of the tongue, and laterally by
the pillars of the fauces, the palatoglossal and palatopharyngeal arches. The isthmus of the fauces is the short constricted space that establishes the connection between the
oral cavity proper and oropharynx. The isthmus is bounded
anteriorly by the palatoglossal folds and posteriorly by the
palatopharyngeal folds. The palatine tonsils, often referred
to as "the tonsils," are masses of lymphoid tissue, one on each
side of the oropharynx. Each tonsil is in a tonsillar sinus
(fossa), bounded by the palatoglossal and palatopharyngeal
arches and the tongue.
Superficial Features of Palate
The mucosa of the hard palate is tightly bound to the
underlying bone; consequently, submucous
injections here are extremely painful. The superior lingual
gingiva, the part of the gingiva covering the lingual surface
of the teeth and the alveolar process, is continuous with the
mucosa of the palate; therefore, injection of an anesthetic
agent into the gingiva of a tooth anesthetizes the adjacent
palatal mucosa.
Deep to the mucosa are mucus-secreting palatine
glands. The openings of the ducts of these glands give the palatine mucosa a pitted (orange-peel)
appearance. In the midline, posterior to the maxillary incisor teeth, is the incisive papilla. This elevation of the
mucosa lies directly anterior to the underlying incisive
fossa.
Radiating laterally from the incisive papilla are several
parallel transverse palatine folds or rugae.
These folds assist with manipulation of food during mastication. Passing posteriorly in the midline of the palate from
the incisive papilla is a narrow whitish streak, the palatine
raphe. It may present as a ridge anteriorly and a groove posteriorly. The palatine raphe marks the site of fusion of the
embryonic palatal processes (palatal shelves). You can feel the transverse palatine folds and the palatine raphe with your tongue.
Muscles of Soft Palate
The soft palate may be elevated so that it is in contact with
the posterior wall of the pharynx. This closes the isthmus
of the pharynx, requiring that one breathes through the
mouth. The soft palate may also be drawn inferiorly so that it
is in contact with the posterior part of the tongue. This closes
the isthmus of the fauces, so that expired air passes through
the nose (even when the mouth is open) and prevents substances in the oral cavity from passing to the pharynx. Tensing the soft palate pulls it tight at an intermediate level so that
the tongue may push against it, compressing masticated food
and propelling it into the pharynx for swallowing.
The five muscles of the soft palate arise from the base of
the cranium and descend to the palate. Note that the direction of pull of the belly of the tensor veli
palatini is redirected approximately 90° because its tendon
uses the pterygoid hamulus as a pulley or trochlea, allowing it
to pull horizontally on the aponeurosis.
Vasculature and Innervation of Palate
The palate has a rich blood supply, chiefly from the greater
palatine artery on each side, a branch of the descending
palatine artery. The greater palatine artery passes
through the greater palatine foramen and runs anteromedially. The lesser palatine artery, a smaller branch of the descending palatine artery, enters the palate through the lesser
palatine foramen and anastomoses with the ascending palatine artery, a branch of the facial artery. The veins
of the palate are tributaries of the pterygoid venous plexus.
The sensory nerves of the palate are branches of the maxillary nerve (CN V2), which branch from the pterygopalatine
ganglion. The greater palatine nerve supplies the gingivae, mucous membrane, and glands of most
of the hard palate. The nasopalatine nerve supplies the
mucous membrane of the anterior part of the hard palate. The lesser palatine nerves supply the soft palate. The palatine nerves accompany the arteries through
the greater and lesser palatine foramina, respectively. Except
for the tensor veli palatini supplied by CN V3, all muscles of
the soft palate are supplied through the pharyngeal plexus of
nerves.