Main Model
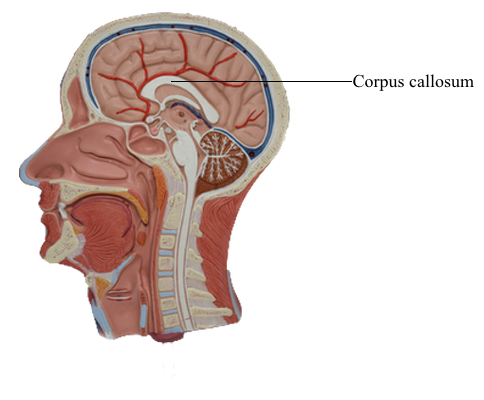
Brain : 4 Corpus callosum
WHITE MATTER OF THE CEREBRAL HEMISPHERE
All information entering or leaving the cerebral cortex or connecting one part of the cortex with another must pass through
the subcortical white matter. In general, the white matter core of
the hemisphere contains association fibers, commissural fibers,
and projection fibers.
Association Fibers
The association fibers interconnect various areas of cortex
within the same hemisphere. These may be short association
fibers that connect the cortices of adjacent gyri or long association fibers that interconnect more distant areas of cortex
(Fig. 16-13). Important examples of the latter are the cingulum located internal to the cingulate gyrus and continuing into
the parahippocampal gyrus, the inferior longitudinal fasciculus (temporal-occipital interconnections), and the uncinate
fasciculus (frontal-temporal interconnections). The superior
longitudinal fasciculus, located in the core of the hemisphere,
interconnects frontal, parietal, and occipital cortices, whereas
the arcuate fasciculus interconnects frontal and temporal lobes
(Fig. 16-13). In the white matter of the temporal lobe, fibers
passing between the frontal and occipital areas make up the inferior frontooccipital fasciculus.
The claustrum, a thin layer of neuron cell bodies located internal to the insular cortex, is sandwiched between two small association bundles (Fig. 16-12). The external capsule is insinuated
between the claustrum and putamen, and the extreme capsule is
located between the claustrum and the insular cortex.
Commissural Fibers: The Corpus Callosum
In general, commissural fibers interconnect corresponding structures on either side of the neuraxis. The largest bundle of commissural fibers is the corpus callosum (Figs. 16-2 and 16-4). This
huge bundle is located superior to the diencephalon and forms
the roof of much of the lateral ventricles. The corpus callosum
consists of, from rostral to caudal, a rostrum, genu, body (also
called trunk), and splenium (Figs. 16-4 and 16-5B). Many of the
fibers passing through the genu arch rostrally to interconnect
the frontal lobes; these form the minor (or frontal) forceps. The
fibers interconnecting the occipital lobes loop through the splenium of the corpus callosum, forming the major (or occipital)
forceps. The tapetum, which is located in the lateral wall of the atrium and posterior horn of the lateral ventricle, is also composed of fiber bundles that cross in the splenium.
Lesions of the corpus callosum, whether the result of surgery or spontaneous, disconnect one hemisphere from the other.
About 80% of patients who have severe generalized seizures
experience significant relief after section of the anterior 75% of
the corpus callosum, largely sparing the splenium. Spontaneous
lesions of the corpus callosum may result from vascular infarct,
tumor (such as oligodendroglioma), or necrosis or demyelination
(as in Marchiafava-Bignami disease). It is recognized that some of
these patients may have a disconnection syndrome.
Smaller commissural bundles include the anterior commissure and the hippocampal commissure (Fig. 16-4). In sagittal
views, the anterior commissure is located caudal to the rostrum
of the corpus callosum but rostral to the main part of the fornix.
This bundle interconnects various parts of the frontal and temporal lobes. The hippocampal commissure is formed by fibers that
originate in the hippocampal formations and cross the midline as
a thin layer inferior to the splenium of the corpus callosum.
The posterior commissure and the habenular commissure
are small fiber bundles traversing the midline that connect caudal parts of the diencephalon (Figs. 16-1 and 16-4). The former
crosses the midline at the base of the pineal gland and just posterior (dorsal) to the cerebral aqueduct. The latter is a small fascicle running along the upper aspect of the posterior commissure
and interconnecting the habenular nuclei.
Projection Fibers: The Internal Capsule
The projection fibers of the hemispheres include both the axons
that originate outside the telencephalon and project to the cerebral cortex (corticopetal) and the axons that arise from cerebral
cortical cells and project to downstream targets (corticofugal).
A prime example of the former are projections from the thalamus to the cerebral cortex (thalamocortical fibers); examples of
the latter are corticospinal, corticopontine, and corticothalamic
fibers. Projection fibers are organized into a large, compact bundle called the internal capsule (Fig. 16-14), which has intimate
structural associations with the diencephalon and basal nuclei.
Consequently, to divide the internal capsule into its constituent
parts, reference must be made to these adjacent cell groups.
In an axial plane through the hemisphere, the internal capsule
appears as a prominent V-shaped structure with the V pointing
medially (Figs. 16-14 and 16-15). It is divided into three parts:
(1) an anterior limb insinuated between the head of the caudate
nucleus and the lenticular nucleus, (2) a posterior limb located
between the dorsal thalamus and the lenticular nucleus, and (3)
a genu located at the intersection of the anterior and posterior
limbs, which is located approximately at the level of the interventricular foramen (Fig. 16-14).
The anterior limb of the internal capsule contains
thalamocortical-corticothalamic fibers (collectively called the
anterior thalamic radiations) that interconnect the dorsomedial
and anterior thalamic nuclei with areas of the frontal lobe and the
cingulate gyrus. Frontopontine fibers, especially those from the
prefrontal areas, also pass through this structure.
The genu of the internal capsule contains corticonuclear
fibers that arise in the frontal cortex just rostral to the precentral
sulcus and from the precentral gyrus (primary motor cortex) and
project to the motor nuclei of cranial nerves. Lesions of these
fibers give rise to motor deficits of cranial nerves, most notably
deficits related to the facial and hypoglossal nerves.
The posterior limb of the internal capsule is larger and more
complex (Fig. 16-14). It is sometimes divided into a thalamolenticular part (located between the thalamus and the lenticular
nucleus), a sublenticular part (fibers passing ventral to the lenticular nucleus), and a retrolenticular part (fibers located caudal
to the lenticular nucleus). However, contemporary terminology
and common usage refer to the thalamolenticular part as the
posterior limb, the sublenticular part as the sublenticular limb,
and the retrolenticular part as the retrolenticular limb. This terminology is considerably less cumbersome and much easier to
remember and is the convention followed here (Figs. 16-14 and
16-15). By this scheme, the internal capsule consists of five parts:
anterior limb, genu, posterior limb, sublenticular limb, and retrolenticular limb.
The major fiber populations passing through the posterior,
sublenticular, and retrolenticular limbs of the internal capsule are summarized in Figure 16-14. Included in the posterior limb are corticospinal fibers arising from the motor
cortex and projecting to the contralateral spinal cord and
thalamocortical-corticothalamic fibers (as part of the central
thalamic radiations) that interconnect nuclei of the dorsal
thalamus with the overlying cortex. Studies in humans have
revealed that corticospinal fibers are somatotopically arranged
in about the caudal half of the posterior limb. Geniculotemporal radiations (auditory radiations) convey auditory information from the medial geniculate nucleus to the transverse
temporal gyri through the sublenticular limb. Visual input from
the lateral geniculate body to the occipital cortex is conveyed
via geniculocalcarine radiations (optic radiations) through the
retrolenticular limb (Fig. 16-14). Optic radiations form a distinct lamina of fibers immediately lateral to the tapetum as
they course caudally into the occipital lobe.
Fibers of the internal capsule flare out into the hemisphere as
they pass distal to the caudate and putamen. This abrupt divergence of internal capsule fibers forms the corona radiata (“radiating crown”), which contains converging corticofugal fibers as
well as diverging corticopetal fibers (see Fig. 16-20).